Another post inspired by lectures in the Memorial Sloan Kettering Oncology Acupuncture course*
What if the treatment that is supposed to save you causes so much suffering that you just want to quit?
"Patients with cancer often fearfully anticipate the prospect of many potential negative consequences resulting from antineoplastic chemotherapy. At or near the top of their concerns is the common adverse effect (AE) of chemotherapy-induced nausea and vomiting (CINV).
"When CINV goes untreated, it affects upwards of 60% to 80% of patients with cancer. CINV not only negatively impacts the quality of life (QOL) of the patient, but also the QOL of the patient’s family. Without prevention and control of CINV, patients may experience many undesirable events that can affect their QOL and/or treatment outcomes, including discontinuation of chemotherapy, which highlights the need for adequate prevention and control measures." (link)
Management of nausea and vomiting in this population is sometimes a matter of life and death. Slightly less dire is the scenario in which it becomes "merely" an appallingly distressing symptom -- one so severe that physical symptoms can be triggered by association and appear in anticipation of the next scheduled administration of chemotherapy.
Current anti-nausea guidelines include NK1 and 5-HK3 receptor antagonists, corticosteroids, and antipsychotic medication. The level of clinical research evidence for the efficacy of these drugs is high, and the benefits are considered to outweigh the harms.
How does acupuncture compare to these top-line drugs? Can we compare them head-to-head, putting aside the common side effects of the pharmacological medications?
The most recent overview of systematic reviews (from 2017), published in the Nature research journal Scientific Reports, concludes that "In the context of current best practice, acupuncture and related therapies may be considered as additional treatments to the guideline-recommended treatment with glucocorticoids, 5-HT3 antagonists and/or NK1R antagonists in patients with moderate or high risk of emesis."
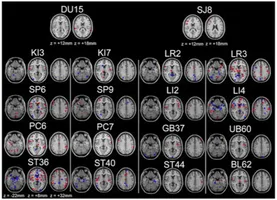
Diving into the studies comparing acupuncture to standard care summarized in that article, a 2006 Cochrane review concluded that acupuncture reduced incidence of vomiting, but not acute or delayed nausea severity, and added that "[this] review complements data on post‐operative nausea and vomiting suggesting a biologic effect of acupuncture‐point stimulation."
It does not appear that there is evidence to support the acupuncture being superior to the standard regimen of receptor antagonists, steroids, and antipsychotics.
This takes us back to the original question -- how effective is acupuncture?
Although acupuncture is not as effective in controlling nausea and vomiting as the top-line pharmacological medications, it has been proven to be effective compared to placebo.
It also has the singular advantage of producing no negative side-effects, unlike common anti-nausea drugs, which include Zofran (constipation, headaches), Emend (fatigue, hiccups), Decadron (insomnia, hyperglycemia), etcetera.
In conclusion, for individuals who:
1) Do not tolerate standard anti-nausea medication well,
2) Tolerate medication but are getting minimal relief, or
3) Do not want to take additional medication...
Acupuncture is a safe, effective, evidence-based option for symptom relief and improving qualify of life!
*Oncology Acupuncture for Chemotherapy-Induced Nausea and Vomiting, with Gary Deng, MD, PhD and Matthew Weitzman, LAc
What if the treatment that is supposed to save you causes so much suffering that you just want to quit?
"Patients with cancer often fearfully anticipate the prospect of many potential negative consequences resulting from antineoplastic chemotherapy. At or near the top of their concerns is the common adverse effect (AE) of chemotherapy-induced nausea and vomiting (CINV).
"When CINV goes untreated, it affects upwards of 60% to 80% of patients with cancer. CINV not only negatively impacts the quality of life (QOL) of the patient, but also the QOL of the patient’s family. Without prevention and control of CINV, patients may experience many undesirable events that can affect their QOL and/or treatment outcomes, including discontinuation of chemotherapy, which highlights the need for adequate prevention and control measures." (link)
Management of nausea and vomiting in this population is sometimes a matter of life and death. Slightly less dire is the scenario in which it becomes "merely" an appallingly distressing symptom -- one so severe that physical symptoms can be triggered by association and appear in anticipation of the next scheduled administration of chemotherapy.
Current anti-nausea guidelines include NK1 and 5-HK3 receptor antagonists, corticosteroids, and antipsychotic medication. The level of clinical research evidence for the efficacy of these drugs is high, and the benefits are considered to outweigh the harms.
How does acupuncture compare to these top-line drugs? Can we compare them head-to-head, putting aside the common side effects of the pharmacological medications?
The most recent overview of systematic reviews (from 2017), published in the Nature research journal Scientific Reports, concludes that "In the context of current best practice, acupuncture and related therapies may be considered as additional treatments to the guideline-recommended treatment with glucocorticoids, 5-HT3 antagonists and/or NK1R antagonists in patients with moderate or high risk of emesis."
Diving into the studies comparing acupuncture to standard care summarized in that article, a 2006 Cochrane review concluded that acupuncture reduced incidence of vomiting, but not acute or delayed nausea severity, and added that "[this] review complements data on post‐operative nausea and vomiting suggesting a biologic effect of acupuncture‐point stimulation."
It does not appear that there is evidence to support the acupuncture being superior to the standard regimen of receptor antagonists, steroids, and antipsychotics.
This takes us back to the original question -- how effective is acupuncture?
Although acupuncture is not as effective in controlling nausea and vomiting as the top-line pharmacological medications, it has been proven to be effective compared to placebo.
It also has the singular advantage of producing no negative side-effects, unlike common anti-nausea drugs, which include Zofran (constipation, headaches), Emend (fatigue, hiccups), Decadron (insomnia, hyperglycemia), etcetera.
In conclusion, for individuals who:
1) Do not tolerate standard anti-nausea medication well,
2) Tolerate medication but are getting minimal relief, or
3) Do not want to take additional medication...
Acupuncture is a safe, effective, evidence-based option for symptom relief and improving qualify of life!
*Oncology Acupuncture for Chemotherapy-Induced Nausea and Vomiting, with Gary Deng, MD, PhD and Matthew Weitzman, LAc